surprise billing
p39, (and chapter 6 too), reading a note about a 2015 study that found, 30% of plans on federal marketplqce, wow, without any emergency physician coverage?!
so all those would be out of network.
cost sharing
p40, cost sharing like HDHP, intended to reduce cost by getting people to shop around more. RAND, findings, less money spent but not by shopping around but by getting less care .
managed care
p41, referrals and prior authorizations, to pay less for services as a respknse to more services and higher costs in 1970s and 1980s?? HMOs. And Medicare Advantage.
More paperwork for clinicians. And more hoops for patients.
churn
p42, hmm, plan churn, disincentivizes insurers from helping with preventative care! some other insurer getting bentfit of better outcome. yikes.
MA: 8% to 33% churn.
only 15% of payroll taxes fund medicare these days
p47, wow!
“since 1965, spending has far exceeded whqt beneficiaries have cojtributed in taxes.”
Cubanski J, Neuman T, Freed M. The facts on Medicare spending and financing. Kaiser Family Foundation. Published August 20, 2019. https://www.kff.org/medicare/issue-brief/the-facts-on-medicare-spending-and-financing/
Ah, ok reading more on that kff.org website, so , ok the other 46% that does not come from pqyroll taxes or premiums , comes from general revenue. (probably just printing fresh debt?)
“Funding for Medicare, which totaled $888 billion in 2021, comes primarily from general revenues (46%), payroll tax revenues (34%), and premiums paid by beneficiaries (15%).”
Dang,
CBO projects that between 2021 and 2032, net Medicare spending—after subtracting premiums and other offsetting receipts—will grow as a share of both the federal budget, from 10.1% to 17.8%, and the nation’s economy, from 3.1% to 4.3% of gross domestic product (GDP). Projected spending growth for Medicare is due in part to growing enrollment in Medicare related to the aging of the population, increased use of services and intensity of care, and rising health care costs.
Fascinating, so Part B outpatient services gobbling up costs , and Part A, emergency services going down,
more from the kff.org link,
Spending on benefits under each part of Medicare (A, B, and D) increased in dollar terms between 2011 and 2021, but the distribution of total benefit payments by part has changed over time. Spending on Part B benefits, including physician services, hospital outpatient services, physician-administered drugs, and other outpatient services, increased from 41% in 2011 to 48% in 2021, and now accounts for the largest share of total spending on Medicare benefits (Figure 4). The share of total spending on Part A benefits (mainly hospital inpatient services) decreased from 47% to 39%, reflecting a shift from inpatient to outpatient services.
medicaid is paid similarly to MA
p50, medicaid managed care plans, are paid, a flat annual fee per beneficiary, in a particular state, and hmm, then they set their own rates with providers.
And up to providers to take or not take medicaid, though not sure how that is switched on/off yet.
Hmm, hospitals get more? Cunningham P, Rudowitz R, Young K, et al. “Understanding Medicaid hospital payments and the impact of recent policy changes.” Kaiser Family Foundation. Published June 9, 2016. https://www.kff.org/report-section/understanding-medicaid-hospital-payments-and-the-impact-of-recent-policy-changes-issue-brief/
Kaiser Family Foundation. Federal Medical Assistance Percentage (FMAP) for Medicaid and multiplier. 2022. https://www.kff.org/medicaid/state-indicator/ federal-matching-rate-and-multiplier/?currentTimeframe=0&sort-Model=%7B%22colId%22:%22Location%22,%22sort%22:%22asc%22%7D
effeft of ACA on Employer Sponsored Insurance
p 53, hmm ESI was 70% of insured individuals in 2009 and 50% in 2019, absorbed by ACA marketplace (or medicaid?).
employers like ESI because of tax benefit 🤦♂️
p54 What Employer pays employees through insurance premium, they can deduct from their corporate taxes and so they can keep the total compensation package to an employee the same but less taxes if they put some into insurance premiums as opposed to the wages. 🤯
p54 however ESI is required by law for companies with ovrr 50 head count. ok.
insurers like it because the pool will be relatively healthy.
Hmm, note here that health care costs are rising and we see wages lagging behind premiums .
Kaiser and capitation plans
p 56, . They are one of the new (?) insurer plus provider models .
oregon medicaid experiment
p57 lottery, organic experiment, mixed results. More access to care, but also no improvement in health outcomes (lipid markers), however some point out it was too early to tell that which takes a long time to measure. And short term, sounds like people were more financially stable, which sounds great. There was increased use of Emergency use even for non emergency needs, but that can happen anyway with private insurance too. Maybe it takes quite a lot more effort to solve that sub-problem, especially since there is a stigma against preventative care.
Baicker K, Finkelstein A, Allen H, et al. Oregon health insurance experiment-results. National Bureau of Economic Research. Accessed April 25, 2022. https://www.nber.org/programs-projects/projects-and-centers/oregon-health-insurance-experiment/ oregon-health-insurance-experiment-results
uninsured: buy now pay later
p60, $42.4 billion for uncompensated, non reimbursed spending, for uninsured. 20% providers ate, 2017, rest government ate it. Authors argue the country chooses to not pay for universal coverage but it is kickijg the can down the road and medicaid ends up footing the bill anyway but probably higher as Emergency dollars.
Monies
p67 nice cashflow charts , for the 4 trillion. Uwe Reinhardt.
Wow, 5% of people initiated 50% of total spend?! three million people , average of $127,284 a year. wow.
Bottom 50%: just 3.2% of spend.
But the growth is decelerating?
Figure 3.3 Wager E, Amim K. How has U.S. spending on healthcare changed over time? Peterson-KFF Health System Tracker. Published February 25, 2022. https:// www.healthsystemtracker.org/chart- collection/u-s-spending-healthcare- changed-time/ #:~:text=From%201970%20through%2
Mayhe slowijg, but still faster than rest of economy
skin in the game and moral hazards
p 70 , so does the style of insurance, where you don’t see the piles of money moving around when you participate in it, make you more wreckless? Is it like a seatbelt effect?
Do people treat insurance like a endless buffet like some may imagine?
Personally, on a HDHP, Im much more penny pinching with utilizing care because I know it is my money but I realize that probably meqns I don’t make use of preventative care which could end up being a overall savings in the long run!
real cost is not known
p 71 quote from RWJF
Little is known about how prices are derived. The answer to the basic question of what health care - costs often is unknown. Payers see a bill, but generally are given very little detail abour how prices in that bill are determined Medpac. Skilled nursing facility services payment system. Revised November, 2021. https://www.medpac.gov/wp-content/ uploads/2021/11/medpac payment basics 21 snf final sec.pdf
healthcare consumer choices are not like the rest of the economy consumer choices
p 73
I have been thinking about this whole, “knowing the pricetag in advance " thing and the authors have a good point about this, with a hypothetical example of a 75 year old mother at a hospital with an inflamed gall bladder. They write,
When you buy groceries, all of your spending is known in ad-vance, but that’s not the case with health care. Further, even if you could know how much it would cost you ahead of time, would that change her or your choices? Would she decide not to have gallbladder sur-gery? Would she risk leaving for another hospital?
If anything maybe it is like Uber Lyft surge pricing?
The authors say buying health insurance is therefore not really like buying broccoli like Justice Anthony Scalia has compared it to.
p76, authors point out the lack of price transparency and lack of choice of what insurance you have if employer based, and lack of choice Emergency Departments have in treating patients, and finally lack of choice in getting ill or getting hit by a car makes the insurance system not really a typical economic market.
(I know some argue we all make choices affecting our health but I think the point is say if you are at the time you are having a myocardial infarction for eating too many doughnuts in the last thirty years, but then at that point in time, you probably will not be comparison shopping).
Fee For Service vs Value Based or Capitation Reimbursement
p 74, interesting inverse point, that yes although Fee For Service incentivises providers to provide more services to get paid more, however, the opposite is true for capitation, that providers are incentivized to provide fewer services.
Realizing that measuring “value” or “quality” or “outcomes” is probably really tricky!
I like authors electrician analogy, for electrician who gets paid for lowering peoples bills. They might not help you if they predict you hqve not much to lower compared to someone else .
aside: prediction is error prone too
Realizing this book pairs well with the AI Snake Oil book too haha.
Medicare reimbursement is leading
Hmm sounds like private insurers model (or copy?) what they do after Medicare? For simplicity?
Oh and Medicare is aiming to move to Value Based care?
CPT codes
p 75 , Current Procedural Terminology. (1960s terminology).
diagnostic or therapeutic service like xray, office visit, or biopsy or earwax removal. hmm also counseling on alcohol misuse.
Oh wow AMA makes $72 million for selling the code book!??!
ohh, all CPT is , is the “what” but “why” is diagnosis, standardized by ICD, ICD-10 with 100,000 diagnoses! Oh wow!
p76 And insurers have rules setup , so that diagnoses ICD codes must be linked to CPT codes for payment to process otherwise denied.
Example in book,
“Z13.82 screening for osteoporosis " and “Z78.0 Asymptomatic Menopausal State”.
Coder arms race?
Sounds like given the complexity, there is a new profession/occupation, of people who translate clinician notes to codes.
And I’m aware this is an area of NLP as well.
Definitely like in 5th Element, Zorg’s chaos translating into profit 😆.
DRG: Medicare’s Prospective instead of Retrospective hospital reimbursement model
DRG or Diagnosis-related Group is a system used by medicare for inpatient hospital classification, of intake, to determine the cost up front as opposed to after the fact.
Inputs:
- type of admitting diagnosis
- severity of condition
- whether a procedure took place
- other known conditions (hmm possible complications ?)
Example given in book is that a myocardial infarction without complications is typically $4,274.25 but more than double otherwise, $9,580.68 . Wow!
This has influenced a reduction in average hospital stay, since it is not a “we will pay you per day” kind of thing .
But wow so much nuance, authors point out that increased hospital stay has consequences other than just a higher bill, like hospital related diseases , and medical errors, both of which are a real thing, also mentioned in The Price We Pay.
In response, a hospital may perhaps on purpose or unwittingly upcode someone, increasing the secerity to increase the expected payment.
stanford alleged billing fraud
“Stanford hospital accused of alleged $468 million dollar healthcare billing fraud: DOJ filed its statement of interest in federal court. " AP News. Published June 19, 2020. https://apnews.com/press-release/prcom/ business-72b885fd050ba0f7512f-c942457b3647
Relative Value Unit
p77 RVU, Physician Fee Schedule, annual, from CMS
inputs:
- overhead 🤔
- malpractice insurance costs
- expected effort , known as wRVU
Examples of wRVU given, too. p77
• a 30-minute office visit with a physician is 1.92 wRVUs, • a screening colonoscopy is 3.26 WRVUs, • admitting a complex patient to the hospital is 3.86 wRVUs, • surgery to replace a hip joint is 19.6 wRVUs.
But hmm author mentions activities like talking to patients have no wRVU 🤔. Also neither diagnostics, author writes “thinking”, but hmm just research in general sounds like would not be here?
I wonder how that compares to lawyer billable hours, or billable hours of other industries like contract work.
Apparently in 2021, CMS updated their wRVU to reflect this question, to address “cognitive” vs “procedural” work.
Conversion factor? from RVU to $$dollars? Wow so like credit card reward points or scrum story points in software development?
p78 Hmm, huhh, an interesting point like also in Price We Pay TPWP , that theres a lot of variation in “volume” for services and less in reimbursement rate per service . Hmm does that mean unnecessary?
Upcoding? In TPWP, they would show cliniciand where they fall on a distribution of something like volume of services like amounts cut for melanoma biopsies.
This was effective. We should do more of these Nudge style interventions .
Seeing Dartmouth Atlas Project, charts these trends 👀, Medicare reimburse-ments— by HRR. 2019. https:// www.dartmouthatlas.org/interactive-apps/medicare-reimbursements/#hrr
Medicare fee schedules are take it or leave it
p79 Hmm and for other private insurers sounds like they negotiate with providers?
Interesting, their negotiation is kind of influenced by the Medicare CMS rates?
p80 Here finally reading about how the “charge price” is much higher than negotiated private price (“transaction price”?) , which is hogher than Medicare reimbursement rates for various CPTs.
Cost shifting theory debunking?
Note here hispitals theoretically offset medicare losses against private reimbursements?
Frakt A. Hospitals are wrong for shifting costs to private insurers. The Upshot. The New York Times. Published March 23, 2015. https:// www.nytime.s.com/2015/03/24/upshot/why-hospitals-are-wrong: about-shifting-costs-to-private-insurers.html? rref=upshot&abt=0002&abg=1
So that was studied and debunked? But authors don’t really mention an alternative theory other than it is what it is 😆.
Sounds like, a kind of, “whatever they can get” scenario , makes sense, but I am reading so far that there are kind of no “market rates” often. Or anyway, the market is asymmetric and this book so far doesnt seem to cover the new transparency laws that were passed recently. But even after those laws passed, it seems it will tqke a long time for those numbers to affect behavior because they are not really surfaced.
And of course in emergencies you choose not by dollar usually.
private variation in reimbursement
p80 Hmm, negotiation means what payors pay for services will vary a lot? Even from plan to plan?
Data on knee hip replacement. wow $20,000 to $70,000 , from Baltimore to NYC?
Peterson-KFF Health System Tracker. Published January 13, 2021. https:// www.healthsystemtracker.org/brief/ price-transparency-and-variation-in-u-s-health-services/
vs chargemaster
ahhh ok cool, so this book was published after the 2021 chargemaster legislation published, so they know about it. Wonder about No Surprise Act timing .
nytimes had discussed colonoscopy variation by plan.
- KliffS, Katz J. Hospitals and insurers didn’t want you to see these prices. Here’s why. The Upshot. The New York Times. Published August 22, 2021. https:// www.nytimes.com/ interactive/2021/08/22/ upshot/hospital-prices.html? campaign id=9&emc= edit nn 20210823&in-stance id=38591&nl=the-morning®i id= 69542217&segment id= 66986&te=1&user id=f32bb 8e73ab- са4414430586c0307cd4c
APM
p82 oh providers can choose which metrics they are graded on? weird.
p 83 hmm and can choose which risks to take on? if spending is lower than spending tzrget , you get an upside bonus?
if worse, you can get a downside penalty?
but can choose between 1 sided or 2 sided?
not allowed to cherry pick anymore i think.
use risk adjustment for sycker pools.
Accountable Care Organizations ACOs (a kind of APM)
p84, They are responsible for populations of people, and contract with Medicare or private payers.
I’m reading that a benchmark is determined as to what a population a payor assigns to an ACO should cost. And my interpretation is, the ACO will collect payments for services over time and then at the end of the year, if they are under the benchmark, for the fees they collected, the payer will give them a bonus which is a portion of the difference, but if they go over, they have to pay the payer part of the difference in the form of a penalty. And they only get the bonus if quality metrics are met. Oddly enough though there doesn’t seem to be a penalty for poor quality. Hmm however they might be removed for poor performance. And maybe more important to the ACO and providers, those quality metrics are publicly available!
In reality, the front line providers collect those fees for services and reconciliation happens at the end of the year.
And again there are ACOs that are upside only or 2-sided. That distinction is made up front.
p 85 Reading that , in 2020, a Medicare ACOs split a mutual savings of $4.1 billion with Medicare, getting to pocket a little more than half. And also for 2020, 97% of Medicare ACOs met the CMS quality ratings that are the post-condition to verify they are not just skimping on care.
So, there is a population, and someone comes up with an expected cost per person which is multiplied by the size of the population. That money is available to the ACO , but I didn’t get yet, does it work like a reimbursement (after the fact) or along the way or before?
Hmmm so, maybe it’s something like, the ACO, provides the various services along the way and does receive fees for those services, but hmm if those fees go over the threshold then they have to give some of it back in the form of a penalty?
Also maybe weird can be that a provider might be playing both games, having an ACO population as well as a separate FFS population along side. Maybe diversification is good?
Reading also https://www.cms.gov/medicare/payment/fee-for-service-providers/shared-savings-program-ssp-acos , maybe Shared Savings Program is the formal name of the CMS program where through the ACA , ACO programs were established.
And it sounds like, as part of an agreement providers negotiate with an ACO they join, at the end of the year, as part of reconciliation, if the ACO gets the quality-adjusted bonus or loss statement from CMS, then that ACO per the agreements would share those bonuses or losses.
Medicare Advantage is not an ACO
Hmm but pool of people is not assigned unlike an ACO but people are advertised to and can sign up on their own during Annual Enrollment Period. When the population is set after enrollment period, then there is a similar process like with ACOs to determine the benchmark for the population, the expected cost. CMS will pay a flat fee, per-member-per-month, hmm a capitation payment.
Unlike an ACO where providers bill CMS directly and reconcile at the end of the year, providers who contract with MA plans will send their claims to the MA plan. ACOs do not process claims like MA middle-men.
p86 Oh wow and sounds like MA plans will attempt to be clever and instead of only pushing to reduce costs will, also push to increase the HCC Hierarchical Condition Category data they provide about patients, so that the risk adjustment formula that CMS runs at the end of the year, comes out higher to bump the benchmark. And the authors cite that to this effect for example, Kaiser was alleged by DOJ in 2021 to have defrauded Medicare of $1 billion, https://news.bloomberglaw.com/health-law-and-business/kaiser-permanente-defrauded-medicare-of-1-billion-doj-alleges .
“CMS pays an average of 4% more per capita for MA beneficiaries than they do for similar patients in traditional Medicare” .
But it sounds like 48% of eligible folks are on MA plans. Authors point out that analyses vary far and wide on this topic. Cherry-picking? So the 4% is real money, but does that mean that the people on MA have better health or is MA a “scam”? This is heavily being debated. Hopefully there can be some way to get a good answer with good evidence everyone can agree on!
Wow I think I just spent an hour and a half trying to understand those 2-3 pages about ACOs and MAs!
SNF Reimbursement
p87 oh Skilled Nursing Facilities, post acute care facilities. You go here hmm, only if three nights in a hospital and go for physical or occupational therapy.
Reimbursement, daily rate, average $434.95
Long term nursing home per diem: not Medicare but Medicaid. $200
..
Big Business ROI
p88 hmm return on investment , if you are attempting to do M&A merger acquisition or middleman types of businesses.
better for pharmacy companies, 18% , not as good for others, drug wholesalers 15% pharmacy benefits managers PBM 12% health insurance plans 12% pharma companies 11% device/tech 10% hospitals in network 7% independent hospital 4.5%
==> from https:/ www2.deloitte.com/content/dam/Deloitte/ec/Documents/life-sciences-health-care/DI Investment-view-of-health-care-market.pdf
Economy of scale?
2018: turning point year, more physicians work for someone as opposed to private practice.! wow
p89 oh wow and hospitals merge into networks. 1990: 65% of regions , very low hospital competition 2016: 90% !!!
Monopolizing?
p90 , analysis northern california vs southern california, when adjusting for wages, (not sure what that means), 20-30% higher sticker prices in the way more consolidated one , north, by Sutter.
inpatient prices 70% , outpatient 17-55% higher,
research from petris.org
As a result, Sutter agreed to settle a monopoly lawsuit for $575 million in 2019! wow. Federal Antitrust lqwsuit still ongoing.
flip side, negotiation with payers can be hard on small practice owners. (p90)
largest
p91 employer with most physicians is United Health
but CVS owns Aetna, which is latgest insurer, huh so larger maybe by revenue but not employees? And CVS also owns two other businesses: mail order pharmacy plus PBM.
PBM
Between big pharma, pharmacies and payers, are PBMs, in the middle.
Price negotiation.
p91 Wow there used to be this thijg where PBMs would tell pharmacies not to tell customers paying out of pocket is cheaper , called a “gag order”. This was banned in 2018. Wow but hmm, what if a PBM also owns the pharmacy too? Like CVS?
Crazy chart showing how a drug costing $17 to produce can cost $100 after all the various wholesalers, PBMs and insurers pocket.
https://healthpolicy.usc.edu/ research/flow-of-money-through-the-pharmaceutical-distribution-system/
Argued point is that yes PBMs negotiate prices down but then dip into the difference to get their cut and how much is the right amount is the question here. Hmm.
Personal opinion, transparency is probably key here, so no asymmetric information as they say.
Why health care so expensive in US
p92.. Oh wow. I think this was already hinted earlier, but per analysys in 2003 Uwe Reinhardt paper, its not that utilization is higher in US, since pvysician visits and hospital days per capita hmm less than OECD median.
But his paper is called “It’s the prices , Stupid!” He doesn’t bury the lead! 😆
information asymmetries
p93 regular people, dont know what things cost. So how could they make proper “rational” decisions?
Not only no “sticker” prices, but also no way to easily “comparison shop” for services.
Rational decisions require access to historical data on averages and extremes and where some hospital or provider in front of you falls on that distribution.
And competition is low anyway these days regionally.
Medical billing is also way more complicated than just a single price anywzy.
There are no people advocating for your wallet. There is a hipocratic oath, for not harming the patient but I think we need one for the wallet too. Though I dont expect clinicians to take that on necessarily.
each billing system is a special unique snowflake
p 94 hmm lack of standardization like in Uk,
A 2011 study, finding , 20.6 hours per physician per week is spent doing health plan stuff , by nurses and PAs, which could have been spent on patient interactions instead. wow. Overhead! extra $82,975 annually!
Interesting point that billing administration for value based care can be more complex than FFS!
sounds to me maybe our HIPAa is causing a cost mess?
p 96 fictional story here authors describe is very telling!
Let’s say Ms. M is admitted to Hospital X for a broken hip after getting hit by a car. She gets a computed tomography (CT) scan, which shows a small brain bleed. After surgical repair of her hip, she’s discharged to SNE, but after a few days she becomes confused and is sent to the ED at Hospital Z. Hospital Z doesn’t have access to her records from Hospital X, so they repeat much of the same blood tests and CT scan of her head. Eventu-ally, she’s discharged home with a home health agency, but the medications from her pharmacy don’t match the med list from Hospital X or from Hospital Z, and she ends up taking too much blood pressure medication. No one has helped her get a timely appointment with her PCP, so she goes to an urgent care, where they don’t have access to any of her records, she doesn’t remember her brain bleed, and they prescribe aspirin. Ms. M’s head bleed thus worsens and she gets confused again, so she’s taken back to Hospital X, where they have no record of anything that happened since she was discharged the first time, and they get a third CT scan. These separate entities-two different hospitals, a nursing facility, pharmacy, doctor’s office, urgent care, and home health agency-do not have any incentive to share information and efficiently coordinate Ms. M’s care.
Authors write about lack of coordination but I suspect HIPAA plays a role too. I recall reading in a statnews article how HIPAA is cited in other situations too, for not revealing how algorithmic discharge decisions are made as opposed to just coordination, but I can imagine it applying here too. 🤔
regulation and cost
p96 , US has less cost regulation unlike other countries (Japan , UK mentioned),
though medicare drug regulation finally arrived in 2022, (Inflation Reduction Act),
but thats just medicare. And a lot of unbounded cost in private.
Authors acknowledge there are tradeoffs to pinning cost of anything of course.
From what Im reading, so far, its the lack of cost transparency and inability to make informed choices about your health even if you did know , that probably contributes most to this wild west of pricing.
low value care
p 97, avoidable spending. generic vs brand name statins, mentioned.
Overtreatment. Acute back pain and use of MRI cited , an area where high cost is used for something that goes away oj its own often.
This reminds me, there is a lot of junk surgery out there too. There was a famous knee replacement placebo surgery study showing one example.
But many others. Also recently saw this former neuro surgeon,
https://youtu.be/25LUF8GmbFU , speaking out about complicated surgeries not really being well understood as helpful and being done. Very specialized and expensive yet potentially also overtreatment!
overuse of ED
also mentioned, going to ED for a cold , or any non urgent thing. Expensive , avoidable.
Related but not mentioned: I realize part of this is there arr people , tens of millions of people, who dont have access to insurance but cannot be refused by ED for when a condition that could have been caught early, gets to be an actual emergency.
expensive longterm chronic conditions
p98, diabetes, cancer, emphysema, asthma, heart disease,
expensive life long treatments 🤔. The system , is it prefering to hold out on cures so we keep paying for longterm treatments?
Diabetes prevalence, from 1% 1960, to 10.5% 2020, wow! Annual medical expenditures can be an additional $9,601, on insulin and other meds.
Hmm wonder how much is Ozempic, Wegowy these days. Wow and diabetes is 3.4% of all health spending!?!
- Kamal R, Kurani N, Ramirez M, Gonzales S. How have diabetes costs and outcomes changed over time in the U.S.? Peterson-KFF Health System Tracker. Published November 15, 2019. https:/ www.healthsystem- tracker.org/chart-collection/ diabetes-care-u-s-changed-time/#item-usdiabetes diabetes-medications-were-second-among-conditions-for-drug-spending-in-2018
end of life care
13% to 25% of Medicare spend, is for last year of life, p99.
social determinants of health sdoh
p100, pollution -> asthma food deserts, medical deserts,
crazy chart! https://www.healthaffairs.org/ doi/10.1377/hlthaff.2018.05187
health care productivity has gone down
p102 . productivity being “output” here like, “number of patients treated per day”, though i dont understand if “treated” means “helped” of just “seen and swindled” 😅.
but if it went down because more individual attention is given yhen that would be good I suppose.
interesting price trendd chart!
…. 2019. https:// www.mercatus.org/system/files/ helland-tabarrok why-are-the-prices-so-damn-high. v2.pdf)
In any case this Baumol effect, says drop in physician productivity is causing the prices to rise .
But what is causing this drop in number of patient interactions?
Another view p103, Alex Tabarrok, economist, is that theres a linear relationship between GDP per capita and health expenditure per capita.
Hezlth cost is probably all of these things, authors summarize.
Sounds like prices are a weird dance between a lot of players, sort of reacting to each other, and with many degrees of freedom since no regulation for private.
Reminds me effect observed , that in 2008-2016 perhaps, the govt fought to increase government loans available to students. It happened, but the also the price of college merely corrected upwards too as if responding to students able to pay more.
quality and delivery
p109, interplay of quality, technology, delivery and reimbursement.
p110, medical quality tracking is born? 1999 report from the Institute of Medicine (IOM) “To Err Is Human: Building a Safer Health System”.
with a quote,
“errors are common, they are costly, systems-related problems cause errors, errors can be prevented, and safety can be improved.”
Was it first report to claim medical error related deaths? 46,000 to 98,000 annually, in US?
Remind me, I was watching HBO Pitt, season 2, recent episode, discussed MERS, which I believe is a bacterial infection more common to spread in hospitals.
My question , since Electronic Health Records mentioned, is HIPAA basically being abused for anticompetetive reasons to prevent medical errors from surfacing, but more so, preventing cost transparency, medical pre authorization transparency, etc?
p110: various categories of medical errors are listed, defined by AHRQ. https://psnet.ahrq.gov
Triple Aim
p112, from Institute for Healthcare Improvement, three aims are , the patient experience, the actual health outcomes, but also the cost.
Menyion of the swiss cheese model of medical errors, of compounding risks. Meaning, how to prevent errors yes, but mitigate when not if they happen.
Donabedian triad
p113, a way to evaluate a system by proxy measures because health outcomes can take a really long time sometimes , to measure.
This suggests outcomes, process, and structure.
Sounds like the input and output.
Process measures, sounds like intermediate outcomes, like how fast were patients seen, maybe, if a lot of medical care is about following protocols and lists of guidelines, you might compare care given to what guidelines recommended.
Sounds also like, in “The Price We Pay”, looking at treatment comparing to distribution of everyone. Their example I recall was centimeters of melanoma biopsy and or removal too.
But sounds like measuring this stuff is super tricky. What if you measure everything but not whether someone washed their hands thoroughly that one time?
Structure, sounds like, staffing and resources available and the finances around this. Interesting, so might eventually see an ROI?
Reporting
p114. Ahh interesting. There will always be errors so relative silence probably means underreporting?
Root Cause Analysis. And hmm maybe literally post mortems? Five whys.
Example in book, CLABSI, cenrral line associated bloodstream infection .
Sounds like lean methodology used in some places.
But unlike in othe sectors, hmm, health care is not blameless right? Because litigation and malpractice insurance are a thing. Proxy measures like always are just that so cant know which ones are important easily.
Sensing potential for measuring what is easier to measure, (p116), which, reminds me of McNamara_fallacy , https://en.wikipedia.org/wiki/McNamara_fallacy .
Yea, but also the checklist idea.
Quality standards bodies
p116, Interestingly it sounds like CMS adapts some of its standards. In particular, they can borrow them from the National Committee for Quality Assurance. They produce a dataset called the Healthcare Effectiveness Data and Information Set. ( https://www.ahrq.gov/learning-health-systems/about.html )
Also reading https://www.ahrq.gov/sites/default/files/wysiwyg/lhs/lhs_case_studies_hca.pdf, a case study on HCA, a private entity that is applying this LHS approach, transforming themselves into a “learning health system”, collecting not just EHR data, but data on any process as well, like they gave an example of a test being ordered, say, whereas originally just the test results would have been part of the EHR, the activity of ordering that test is separately logged.
p116, noting that in 2018, CMS finished spending $1.3 billion over a decade on developing 788 new measures, but there are questions, about how do we know that all of this tracking activity is contributing to actual better patient outcomes (and other aspects of quality too like patient experience, and without increased staff burnout say).
A reference pointing out that 7 out of 33 metrics on CMS are about “patient experience”, https://www.cms.gov/medicare/medicare-fee-for-service-payment/sharedsavingsprogram/downloads/aco-shared-savings-program-quality-measures.pdf
(screenshot from above link:)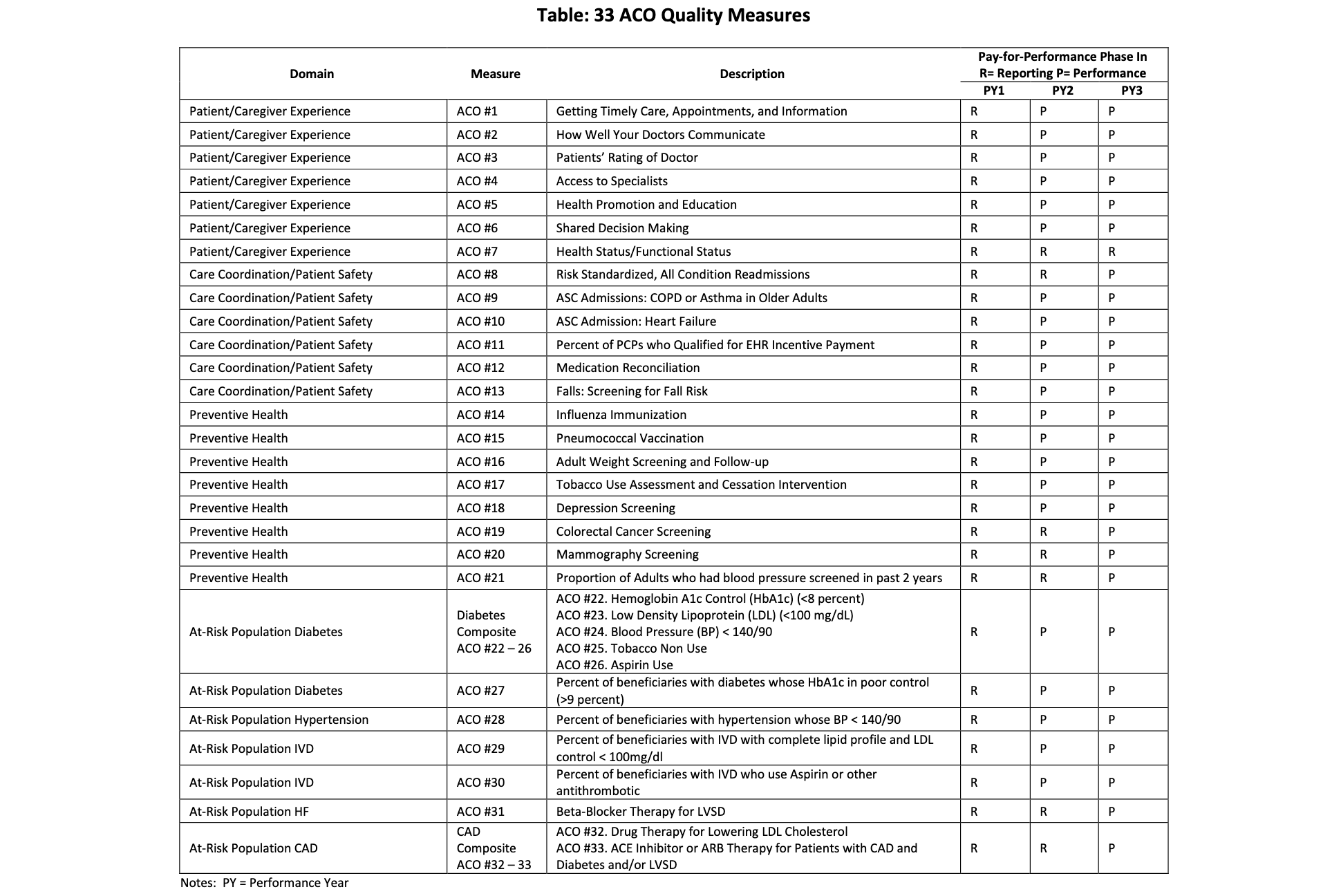
This table is kind of confusing though, why does it have literally just 33 metrics? I thought there were hundreds??
Adverse Drug Events and medication errors
p117, estimated associated with 7,000 deaths a year??! wow
Oh interesting, switching away from handwritten scriprs helped.
And, hmm “med rec”, medication reconciliation, hrlping awareness on drug interactions, especially, hmm, between, different lists a patient might have, w.r.t. different facilities they go to.
Hmm but how does this work, I always wondered how freely doss EHR information flow between your different providers. Why do they constantly ask you for your medical history as if they cannot conceivably get it from your past providers?!? Hope this book explains that! When you see a new provider you are always rushed to remember your history but that is a crazy ask.
Authors write that “med reconciliation " doesnt always happen yet and studies still discover big descrepencies .
Nosocomial infections
p117, infections at a hospital
hmm, risk factors , higher for already being sick, but hmm also IV lines, catheters, hmm, CLABSIs, mentioned a few pages ezrlier.
Oh cool, I didnt realize these are preventable w.r.t. errors, and that using checklists has helped, to improve HAIs, health care associated infections. Due to, Laurance J. Peter Pronovost: champion of checklists in critical care. Lancet, https:// www.sciencedirect.com/ science/article/pii/S0140673609614392
I wonder if this is related to the Checklist Manifesto book, from Atul Gawande, which I remember was given to everyone at my company in 2015, that was a fond memory.
p118, sounds like nevertheless, HAI reduced into 2010s, but still number here , $40billion cost total, hmm ouch. Long way to go!!
Reading, Medicare, uses stick approach, to not reimburse after HAI for certain procedures, ok. I hope there is not a weird self under-reporting consequence then? Sounds really tricky to get reliable data and prevent a conflict of interest here!
handoffs
p118 lots of handoffs for people in hispital . hmm but why is this any different from fact that you have many providers in your life in the grand scheme of things.
although i get that not everyone has a chronic condition.
SBAR, IPASS, hand off standards. cool.
think im starting to see why residents are asked to work crazy hours, maybe to reduce hand off related errors? If we fix this we could reduce fatigue related errors???? 😲
https://www.psgh.com/ news/i-pass-and-sbar-handoff-tools-have-proven-benefits/
chronic conditions
p119, saying we know what are the causes of hypertension (aka high blood pressure ). I didnt know we know, I thought we only knew the risk factors.
This is being discussed next to preventative care because apparently high blood pressure doesn’t have a particular symptom and so checking if you have this would be really good preventative care.
Contributing factors, diet, exercise, smoking, alcohol, sleep, stress, and indirectly, access to medicine to control it, genetics and age.
Hmm well [3] seems to say being over 55 is a risk factor, hmm but has that been true, when controlling for all of the other factors like other disease that might be more common after your 55?
(I recall I had a note about p42 about lack of incentives for insurers to pay for preventative care since insurance has churn which outweighs the benefit . What about bad karma 😆?)
disparities by area
p121, New Orleans example, where localized life expectancy statistics hide behind averages. So New Orleans average of about 77, tracks national average, but 55 for French Quarter,
https://www.rwif.org/en/library/infographics/new-orleans-map.html
Data is by parishes, this term, defined here as, neighborhoods, hoghly segrerated by race and income.
p122, story of Kaiser Permanente, cutting hypertension gap in outcomes , between Black and White populations, in half.
EHR EMR pitfalls
p123, oh wow, crazy, i didnt realize, EHR was purely a federal government thing, in Veterans Affairs since 1990s, and only after, 2009, Health Information Technology for Economic and Clinical Health HITECH Act, percentage of hospitals using EHR surged from 10% to 97% in just 5 years. Wow!!
Epic, Cerner, Meditech, Allscripts, four companies.
https://www.beckershospitalreview.com/ ehrs/ehr-market-share-2021-10-things-to-know-about-major-players-epic-cerner-meditech-allscripts.html
p124, information blocking banned. https://www.healthit.gov/curesrule
p125 Ahhh, finally the explanation about why health records are difficult to connect if you change providers, because indeed, they are not centralized, and patients have to sign a release form for access to each place information. requesting has to happen, it is not automatic.
Im reading EHR by fax, huhh?
a Health Information Exchange, HIE, helps to make the transfers , and there are more than 100 of them?? Huh so they are separate from Epic etc?
oh but Strategic Health Information Exchange Collaborative is a 90% umbrella? https://strategichie.com
p126 dang sounds like there is “sludge” all around here. Vendors of the EHR want to make it hard for health provider systems to switch, and they want to hoard all the nice priprietary data. And those health providers want to be patients’ AOL too, make it hard to switch. Its all about that lockin!
Vendors will try to charge fees for attempts to move data around . Sounds like the Cures Act, was an attempt to penalize these shenanigans.
Reading about Fast healthcare Interoperability Resources FIRE, described on https://www.healthit.gov
Sort of the whole HIPAA thing is used as an excusr for lockin you traditionally see in the rest of big tech.
Although, it does make sense that maybe the health portals did not design them with intent to make it easy to fetch your records as the first use case. I suppose they were primarily for clinicians. Actually these kinds of systems can bloat quickly . Not for lack of trying. There is not much incentive to make a good UI / UX since you want to put money towards the health outcomes theoretically and patient portals are probably an afterthought.
References
- Healthcare Handbook, 3rd edition.
- …
- https://my.clevelandclinic.org/health/diseases/4314-hypertension-high-blood-pressure